Report Excerpts
Black men ages 55-60 serving a sentence post-conviction are the largest impacted population by deaths behind bars, comprising 11% of all known deaths. None of the 786 known deaths were judicially sentenced to death row. All were either detained before their trial, serving a judicially determined sentence for a set number of years or life, or were detained for a parole or probation violation. The overwhelming majority of people died of medical causes, with the highest rates for heart disease and cancer. Approximately half of known medical deaths were related to a pre-existing medical condition, indicating that half of medical related deaths were due to conditions first diagnosed by prison or jail medical staff. Though suicides were only approximately 6% of deaths, they were more likely to occur in parish jails and within those jails, half occurred in segregation, more commonly known as solitary confinement.
Who is Dying?
Race, Sex, Age & Trial Status
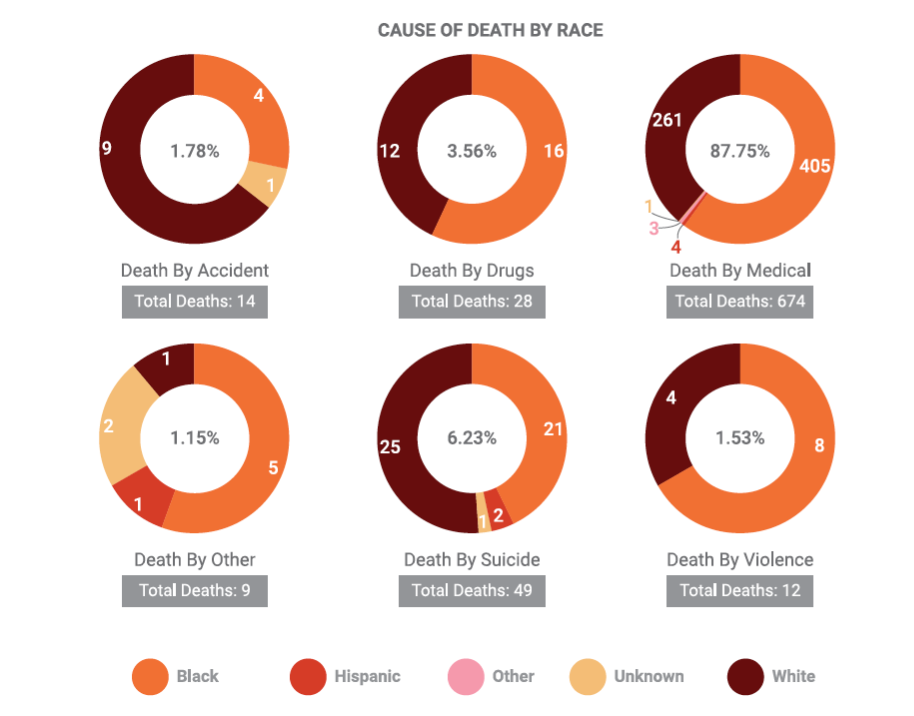
Race
Of the 786 known deaths from 2015 to 2019, Black people were 58.40% (459) of deaths and White people were 39.69% (312) of deaths. Of the remaining 14 deaths, seven were listed as Hispanic and the remaining were either listed as “other” or “unknown.”
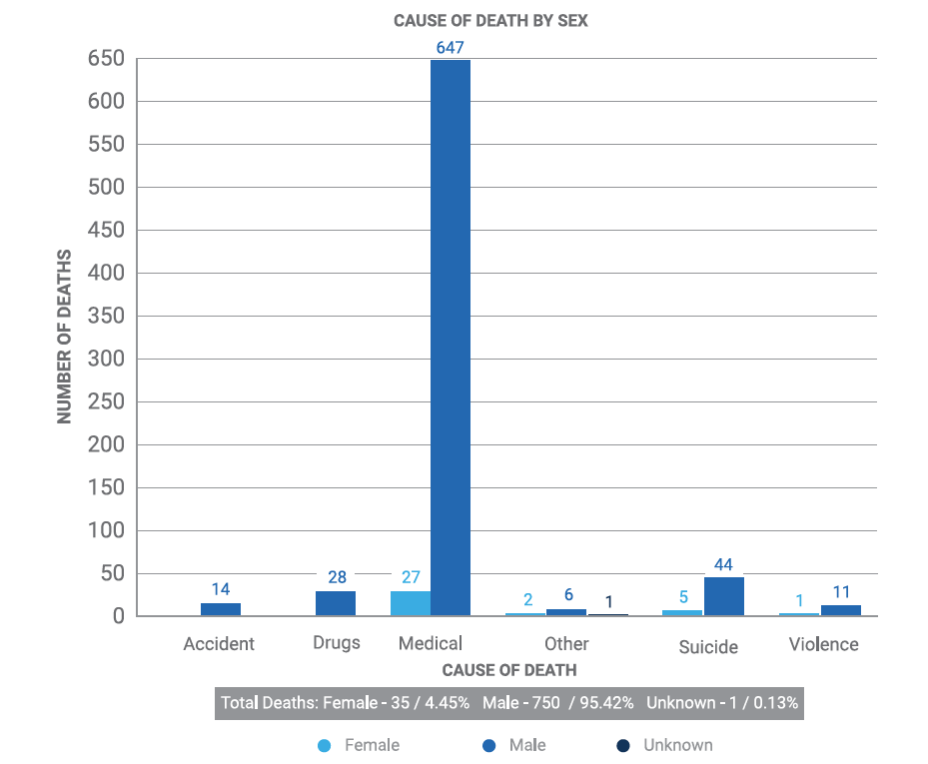
Sex
Of the 786 death records reviewed, 95.42% were for men (750) versus 4.45% for women (35). Medical deaths were the leading cause of death for both men and women, followed by suicide. Deaths as a result of drugs or accidents were exclusively male.
Age
Known deaths behind bars in Louisiana range in age from 13-96 years old. Overall, people ages 55-60 years old make up 19.24% of deaths, with people ages 61-66 at 17.13% and 49-54 at 15.92%.
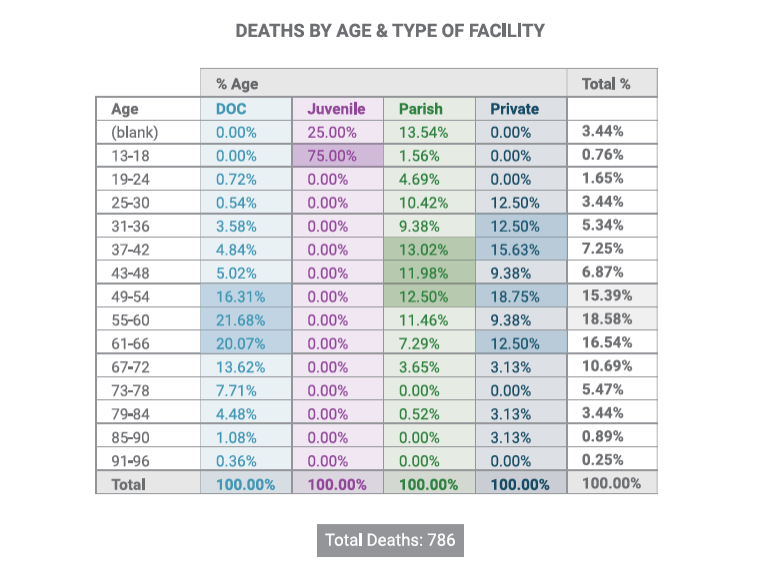
Trial Status
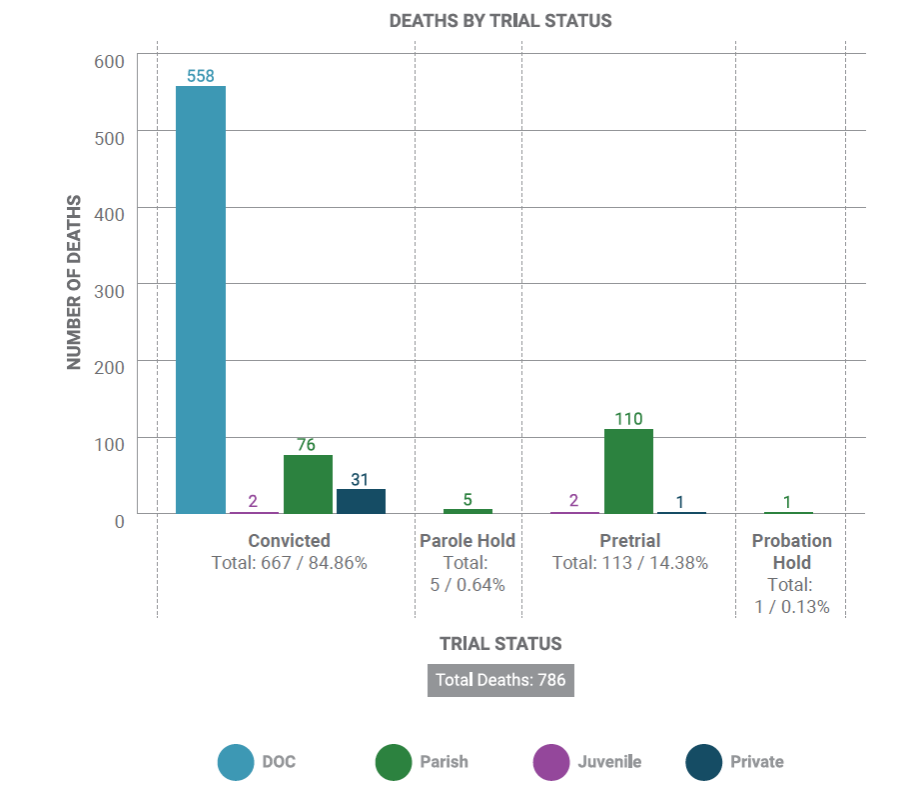
Approximately 85% of known deaths behind bars were of people serving a sentence for conviction of a crime. These deaths occurred primarily within DOC prisons (558 deaths for 70.99% of total deaths), but people with convictions also died serving their sentence in parish jails (76 for 9.67% of deaths), private facilities (31 deaths or 3.94%), and juvenile facilities (2 deaths). Pretrial deaths, i.e. deaths of people who had not yet had a trial determining their guilt or innocence, are 14.38% of all known deaths from 2015-2019, including two juveniles.
Where are they dying?
Type of Facility, Location within Facility
Type of Facility
Louisiana is relatively unique in the U.S. for using local jails to house approximately 50% of people serving their state sentence in a local jail. Jails are traditionally operated by local sheriffs and are primarily for people detained pretrial. They are designed for short-term housing and therefore often lack more robust services essential for people serving long-term sentences, including appropriate healthcare, recidivism prevention programming, and skills training. Prisons, on the other hand, are operated by the state and are primarily for people serving a judicially determined sentence after being convicted of a crime. As a result of this bifurcated system, the DPSC prioritizes state prison beds for people with longer sentences or serious health needs. Local jails and private operators, such as LaSalle Corrections, house the remaining state population of 50%, in addition to their traditional pretrial populations.
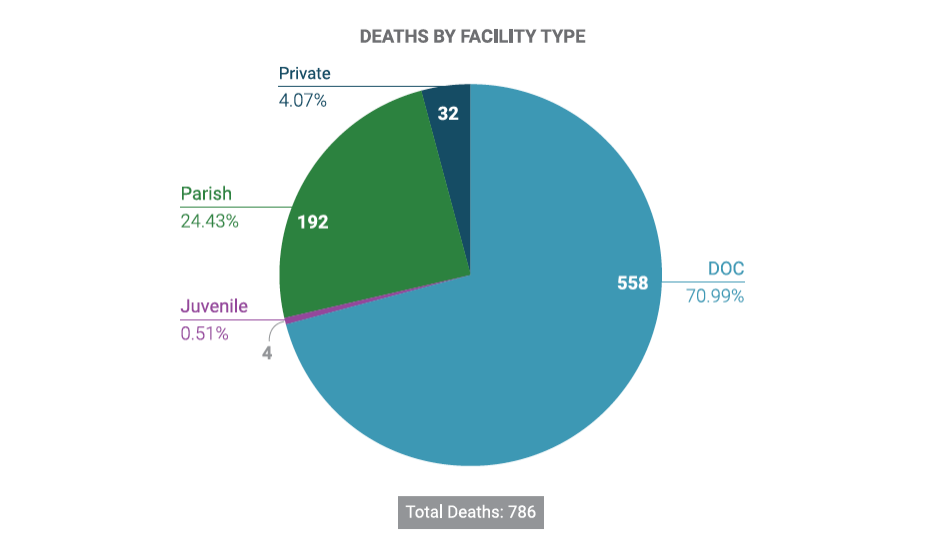
Of the 786 known deaths, the majority occurred within state prisons, though deaths occurred in all types of facilities during the 2015-2019 period of review.
Location of Death within Facility
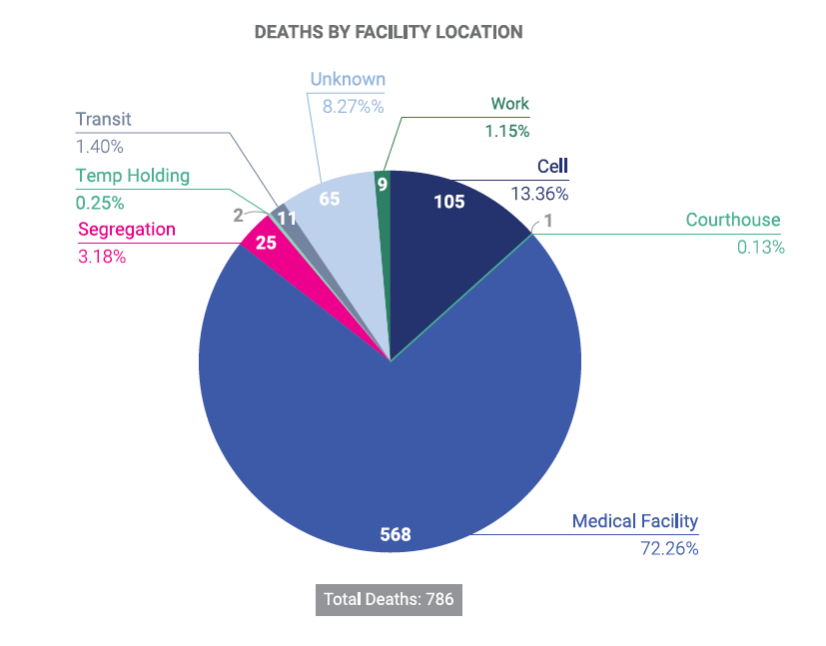
Almost three-quarters of deaths (72.6%) occurred in a medical facility, which is consistent with medical illness being the leading cause of known deaths. While the “unknown” death location appears large, a review of those records indicates the majority of those deaths occurred in medical facilities outside of the prison or jail. Deaths in segregation may indicate challenges for custodial supervision and/or reflect the unique isolation of segregation cells. Segregation, more commonly known as solitary confinement, is usually employed for discipline for rule violations, protective custody, or for close observation/suicide watch. In segregation, a person is typically allowed out of their 6×8 foot cell for 1-2 hours each day, but is otherwise isolated from human interaction, denied visitation or participation in programming, as well as other privileges.
Why are they dying?
Medical, Suicide, Drugs, Accident, Violence
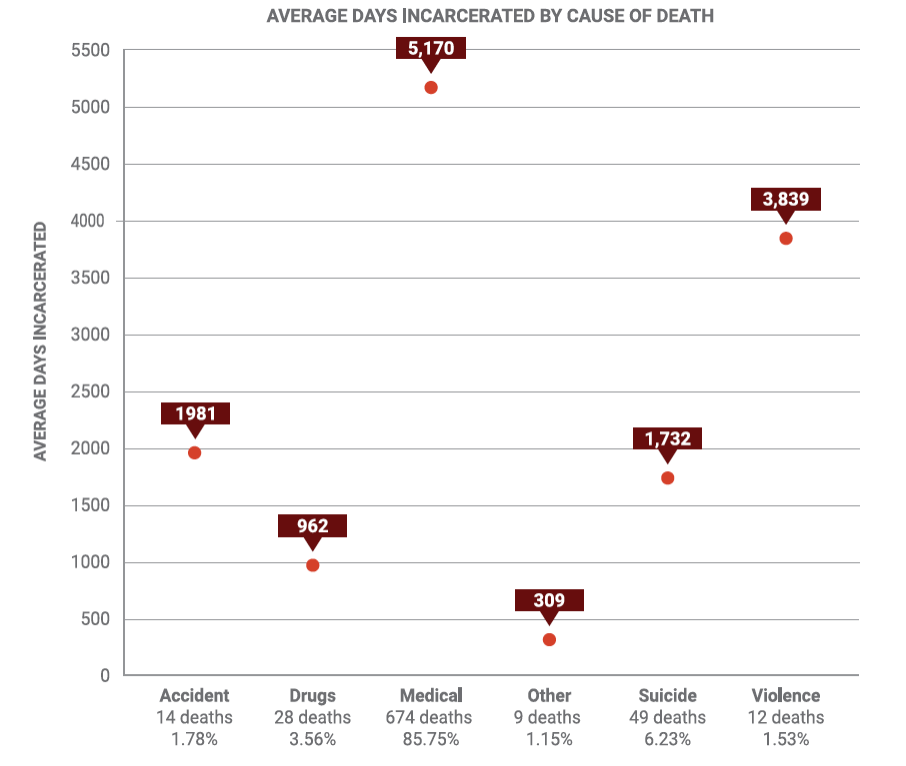
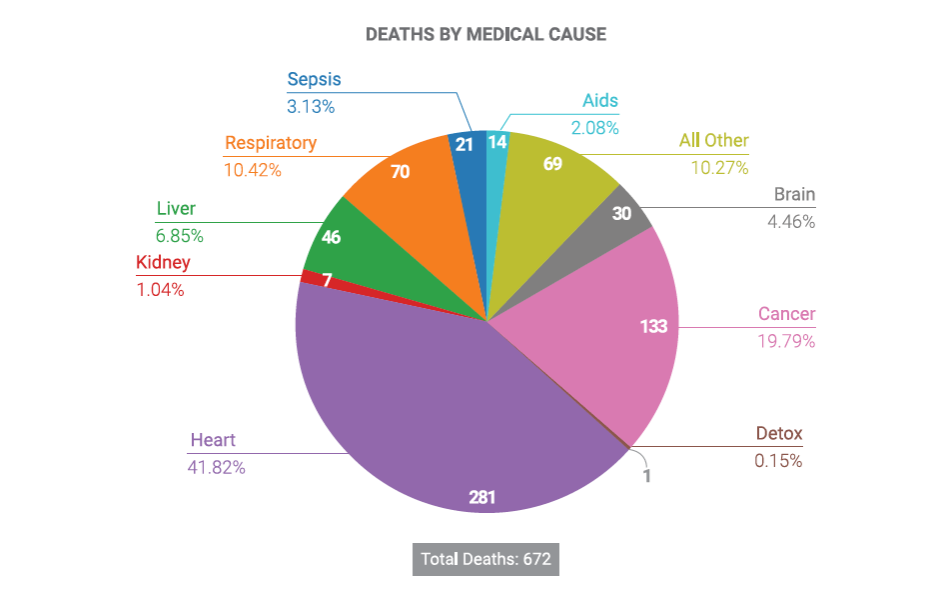
The vast majority of deaths (85.75%) were related to medical illness. Contrary to popular culture depictions of prisons and jails, known deaths due to violence are a relatively small overall proportion of deaths behind bars. The second leading cause of death at 6.23% are completed suicides. Drug overdoses are third at 3.56% and though a small overall proportion of deaths, these overdoses occurred close in time to admission but also after years of being incarcerated.
Medical
The leading causes of medically-related deaths behind bars are cancer and heart attacks. Approximately 10% of known deaths from 2015 to 2019 are due to respiratory illness. Some of the deaths within the “all other” category concern deaths at facilities that either redacted the medical cause of death, failed to provide descriptive details on the cause of death, or described the deaths as the result of “natural causes.” Additional deaths within this category included deaths due to sickle cell, complications from hernia surgery, Alzheimers, and gastric ulcers, among others.
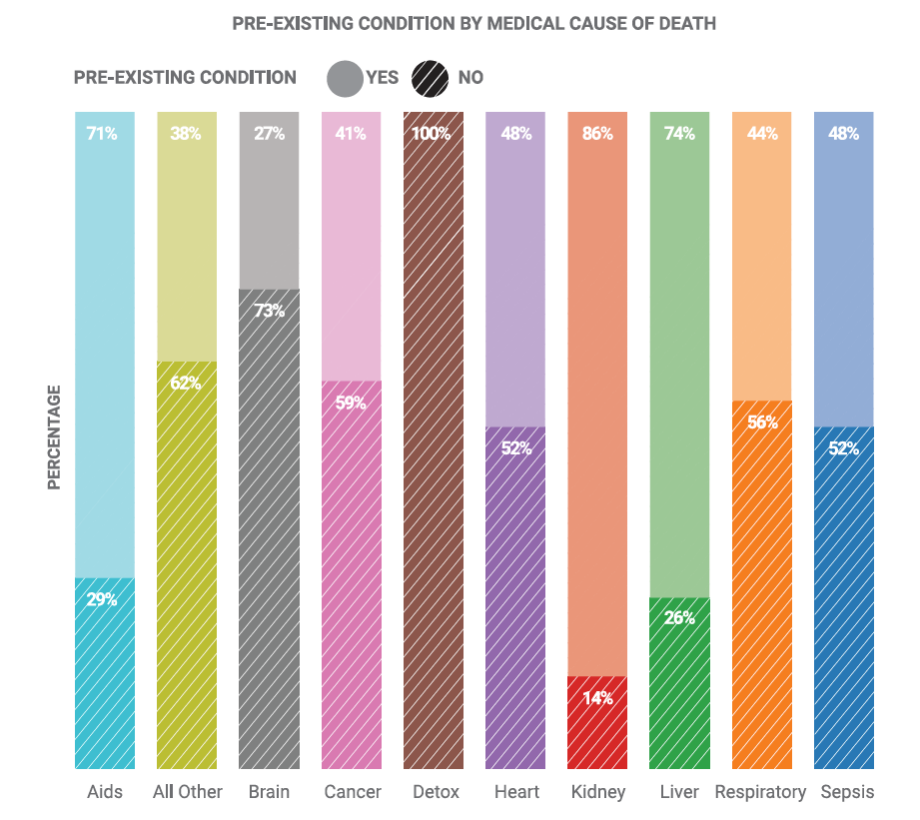
On average, less than half of known deaths were due to a medical condition that existed prior to detention behind bars, indicating that the medical condition in 53% of cases was initially diagnosed after being incarcerated. Only medical deaths due to three diseases (HIV/ AIDS, liver, and kidney diseases) were more likely to be due to a pre-existing condition prior to incarceration. The development of – and death from – other diseases during incarceration is likely related to the length of sentences in Louisiana and may implicate the general lack of preventative health care for incarcerated adults under the age of 50 years old.
Suicide
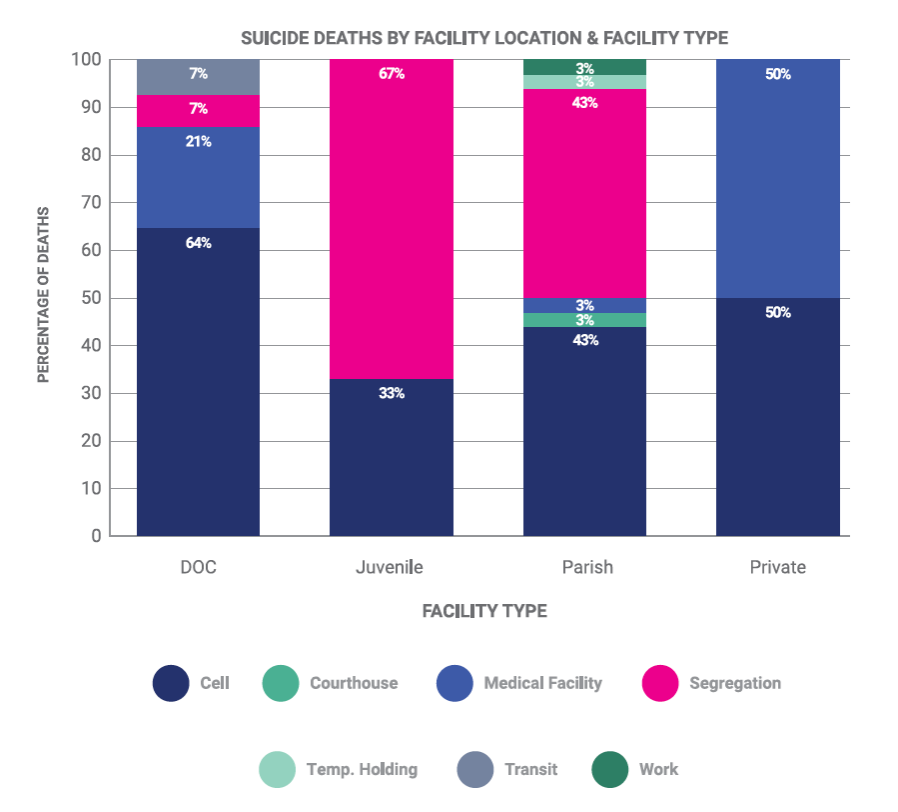
Almost two-thirds of the completed and known suicides in state prisons occurred in a person’s cell and only 7% occurred in segregation. In contrast, suicides in segregation were more common in youth detention centers and parish jails. Suicides in segregation are of particular concern, since segregation settings usually entail a higher level of individual supervision/observation than general shared cell or dorm settings combined with more restrictive policies on items allowed in a segregation cell. Half of all completed suicides in parish jails occurred in segregation cells, raising questions about the degree of observation performed by custodial and medical staff. All but two of these segregation parish jail suicides were hangings.
Drugs
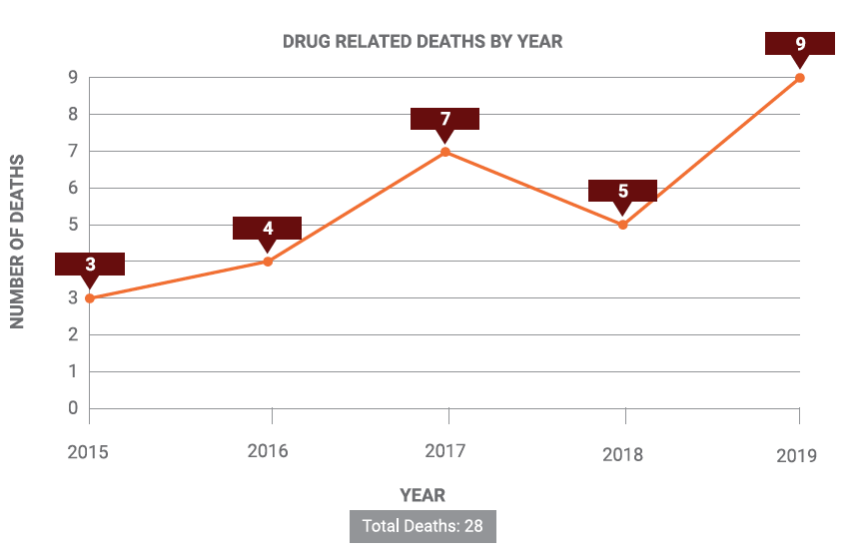
Drug overdoses are a relatively small proportion of overall deaths and similar to suicides, are more likely to occur in parish jails than other types of facilities. Drugs causing death included cocaine, heroin, methamphetamines, fentanyl, ibuprofen, synthetic cannabinoids, and inhaled hydrocarbons.
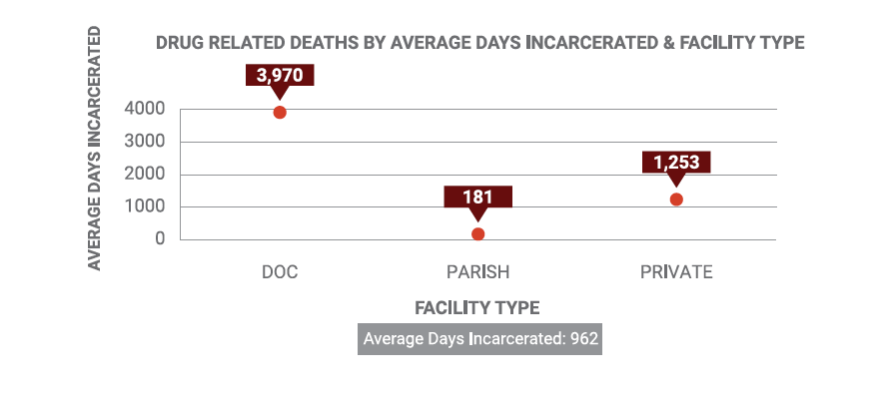
Known drug-related deaths appear to be increasing in number over time. The lowest proportion of drug-related deaths was in 2015 at 1.7% of overall known deaths behind bars. By 2019, drug-related deaths were 7% of overall deaths for the year. All drug overdose deaths behind bars from 2015-2019 are male.
Accident
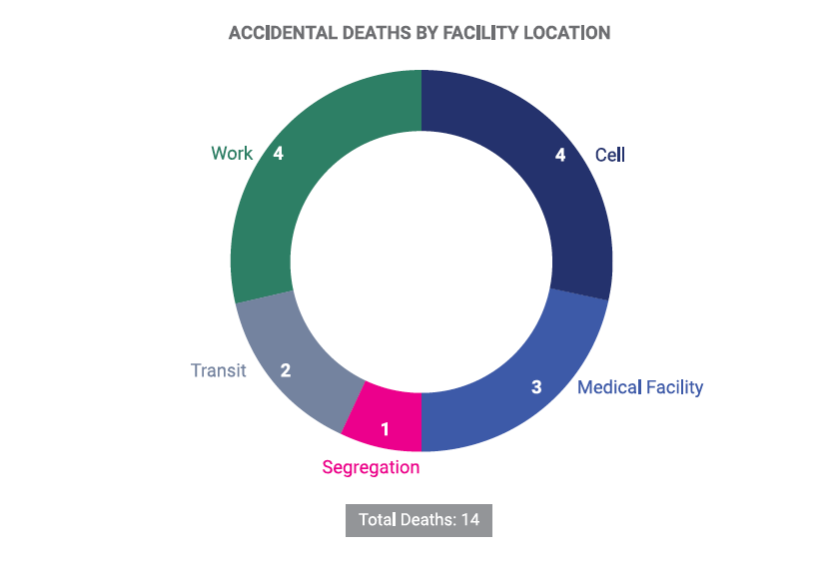
Deaths due to accidents behind bars primarily involved head injuries leading to traumatic brain injuries. One death is reported as “accidental” but concerns an officer-involved shooting after the person’s apparent failure to heed the prior fired warning shot. For deaths in cells, three of the accidental deaths were due to head injuries, of which one is described as the result of falling down. The fourth death did not indicate how the injury leading to death was sustained. Of the four deaths occurring as a result of work, two involved drowning (one when a boat collapsed on the Mississippi River); one involved falling from the bed of a truck travelling down a U.S. highway; and one involved an unspecified “accidental injury to self” at work.
Violence
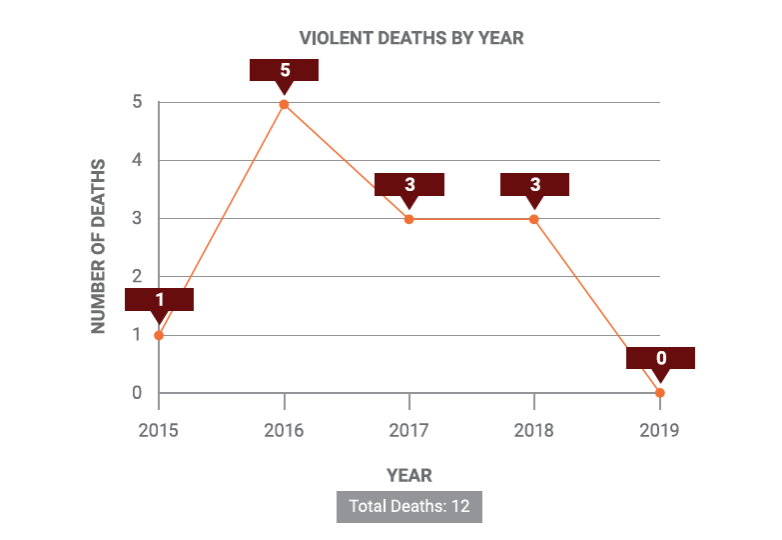
Deaths due to violence were one of the least common forms of deaths behind bars in Louisiana. Two-thirds of deaths due to violence occurred in cells, the majority of which involved assaults and blunt force trauma leading to head injuries. This would seem to indicate that the violence was not a product of contraband or homemade weapons, but does implicate supervision and observation policies of these facilities. The timing of these deaths was evenly spread across morning, afternoon, evening, and overnight. Notably, two of the three reported violent deaths occurring in East Baton Rouge Parish Prison happened in the evening.
Conclusion
While not all deaths behind bars are necessarily preventable, prisons and jails should ideally have lower death rates than the general public due to the physical proximity of medical care behind bars, 24-hour staffing and supervision, and reduced probability of certain types of deaths, such as car accidents, due to incarceration.
A person’s risk of death behind bars should not depend on their facility assignment. Although DOC prioritizes placement of people with serious medical needs in select state prisons, such as Louisiana State Penitentiary, medical-related deaths also occurred in parish jails where there are less robust medical systems in place.
Death behind bars can impact anyone incarcerated, regardless of their crime or guilt or innocence. Some incarcerated people died relatively early in their judicially determined sentences. Others died after completing the majority of their sentence while enrolled in work release programs designed to aid their transition home. Fourteen percent of deaths were of people who had only been accused of a crime, without a chance to prove their innocence, or to be found guilty.
Prison, jail, and youth detention administrators can and should use this data to compare the operation of their individual facilities to others. In some cases, the trends identified implicate institutional policies and practices, which should be reviewed with the aim of decreasing deaths behind bars.
State and local leaders should officially collect, track, analyze, and publish this data for the public. This report can serve as an important baseline for future research and analysis, but continued transparency of our public institutions is needed for sustainable improvements and public support.